
Providing access to Ambulatory Blood Pressure Monitoring (ABPM) for patients can be challenging in primary care. The growing evidence for the prognostic power of ABPM is leading to new approaches to support clinicians with the best data for their patients.
We spoke with clinicians and their patients about a feasibility study into delivering ABPM at community pharmacies with the Oscar 2 Ambulatory Blood Pressure Monitor.
Principal Investigator

Dr. Dave Dixon, PharmD
Dr. Dixon's drive to increase access to ABPM for patients in the US led to a feasibility study at Virginia Commonwealth University in partnership with Bremo Pharmacy.
What led you to set up this service?
I’ve been involved in helping patients manage their hypertension for my whole career. My prior experience with ambulatory blood pressure monitoring was in a study looking at the effect of certain drugs based on the timing of doses during the day. I ran across a paper on increasing access to ABPM through community pharmacies and discussed with other providers in my practice that this was a valuable service that wasn’t available in the US.
What were the goals of setting up the service and study?
We wanted to conduct a feasibility study and to understand whether this model would work in the US. Understanding whether providers would refer their patients was a goal of the study alongside whether pharmacists would be comfortable with conducting ABPM studies. We also wanted to particularly focus on the patient experience of an ABPM service provided by pharmacists. We developed a patient questionnaire to gain information on their experience with not just the monitor, but also with the pharmacist providing the service.
Why is ABPM important to hypertension management?
I’ve seen in my practice the challenge of getting patients to perform home blood pressure readings themselves. Often even if the patient has a monitor and wants to check their blood pressure, we don’t see measurements brought to their appointment or we receive only blood pressure readings from the patient’s memory. In order to address issues of whether that patient has white coat or masked hypertension we need better clinical data.
More importantly, there’s been a lot of literature to support the idea that the 24-hour blood pressure profile and in particular night-time blood pressure predicts cardiovascular risk better than office-based blood pressure. ABPM is the perfect fit for being able to know what is going on with the patient at home and outside the clinical setting.
How does the service work?
We aimed to keep the process simple for the provider, who fills out a referral form we developed. The form is sent to the community pharmacy, who reach out to the patient to schedule a visit. We wanted to ensure we could plan ABPM visits in advance to best manage the pharmacists time and keep it convenient for the patient.
 1. Providers refer their patient to the pharmacy.
1. Providers refer their patient to the pharmacy.
 2. Pharmacy calls patient to schedule ABPM visit at convenient time.
2. Pharmacy calls patient to schedule ABPM visit at convenient time.
 3. A pharmacist tech fits the ABPM to the patient.
3. A pharmacist tech fits the ABPM to the patient.
 4. The report is sent to the patient’s provider.
4. The report is sent to the patient’s provider.
During the patient visit, a pharmacist or pharmacy technician will perform intake and set up the monitor on the patient, providing guidance to the patient.
When the device is returned by the patient, a pharmacist will provide interpretation and recommendations to the referring provider alongside the 24-hour blood pressure report.
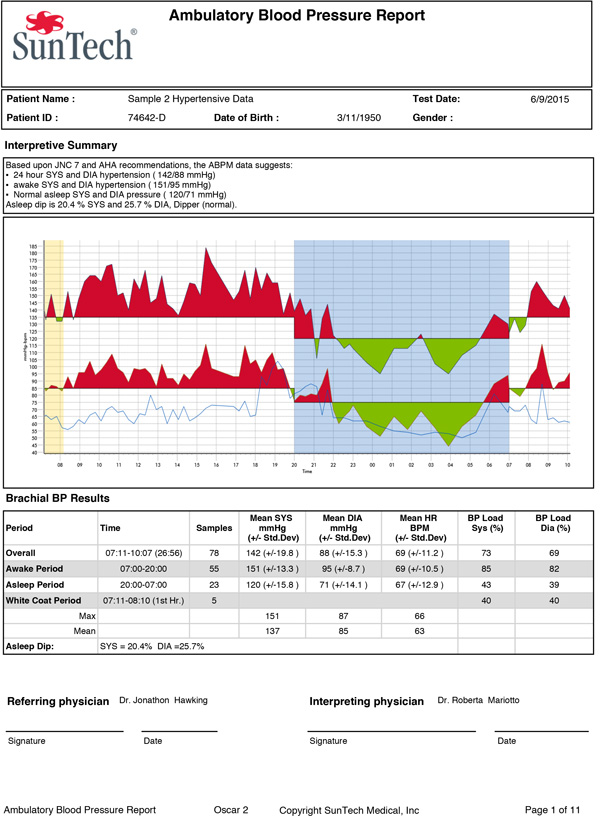
The report provides objective evidence for the patient to say, “OK, wow, I really am hypertensive”. It helps patients to grasp the significance of the condition and may help adherence to treatment.
Oscar 2 24-hour Blood Pressure Report
[Click to Enlarge]
What is the benefit to the patient of the service?
Having your blood pressure taken at the office can be a stressful experience, while self-measuring blood pressure at home can be a great deal of work for patients. ABPM allows the patient to see the full spectrum of their blood pressures, not just during the day, but also at night. Particularly for patients that are not convinced of their high blood pressure, the report provides objective evidence for the patient to say, “OK wow I really am hypertensive”. It helps patients to grasp the significance of the condition and may help adherence to treatment down the road.
How did you recruit providers and pharmacists to refer to your service?
It was very important to have face to face time with providers. We set aside time during lunch periods to visit and talk with providers about ABPM and which patients they would refer to an ABPM service. Fortunately, the response from providers was very favorable. Many of the providers we spoke with wanted access to ABPM but did not have the ability to offer it directly to patients or an established service to refer patients to.
Pharmacists currently play a big role in assisting patients in selecting a home blood pressure device and training patients on taking home blood pressure, but there was less familiarity with ABPM. Pharmacists were enthusiastic about the data provided by a wearable blood pressure monitor and we also provided training to all our pharmacists and pharmacy technicians taking part in the service which helped ensure they were confident in working with ABPM.
“The number of referrals we received from providers really took us by surprise”
What was the reaction from the patient?
Patients really enjoyed learning more about how their blood pressure changes throughout the day. Having the objective graph really helped to either reaffirm a diagnosis of hypertension for the patient or confirm suspected white-coat hypertension.
Patients were typically able to tolerate ABPM well. We went into detail with sleeping arrangements with patients to ensure they understood what to expect during the study and would adhere to the 24-hour study schedule.
A Success Story
An older adult female was concerned about low blood pressure symptoms and was being treated with several anti-hypertensive medications. The patient’s provider was reluctant to reduce her medication regimen based on the patient’s history but referred her to the program to get a better picture of blood pressure.
The patient’s report indicated a 24-hour average of well below normal with significant dips throughout the day indicating the patient was hypotensive. The report allowed the patient’s provider to discontinue some medications and potentially prevent an adverse drug reaction. The patient was extremely pleased to have objective evidence of symptoms and the provider had the confidence to make a change to the patient’s medication.
How did you decide what protocols to follow for ABPM?
There are a lot of recommendations available, however we followed the recommendations of European Society of Hypertension (ESH), particularly for intervals during the nighttime portion of the study.
Was it a challenge for Pharmacists to fit in a new service to provide to patients?
Pharmacists were able to integrate ABPM into their workflow extremely well. Pharmacists are increasingly providing additional healthcare services, particularly immunizations, and the fall can be extremely busy, so we expected integrating a new service to be a challenge. We found that pharmacy technicians were able to take on a larger role in managing the new service which ensured pharmacists could focus on interpreting the ABPM results and spend time providing other healthcare services.
How did you manage reimbursement for the study?
While there is coverage for ABPM from payers, we did struggle with reimbursement due to restrictions on pharmacists directly claiming reimbursement. We are looking at multiple options, such as partnering with a medical group to assist with reimbursement and we also are exploring an out of pocket model for patients with an expectation of a $50 charge for an ABPM study.
Why did you choose the Oscar 2?
I had experience in the past with other monitors where the durability was not great. I also had observed that the usability of the software was often limited. I was aware of the Oscar 2 and searched PubMed for studies using the Oscar 2 and found the usability and durability were highly rated. We also found the cuff sizes on the Oscar 2 were better suited to our patients, with larger cuff sizes to accommodate patients with a larger arm size.
What has been your experience of using Oscar 2?
Oscar 2 has provided the ability to capture readings very consistently throughout the study, certainly better than other monitors I have used in the past. We would absolutely recommend the Oscar 2.
What do you have planned to follow the completion of this study?
We have manuscripts planned to document the development and implementation of the service as well as clinical outcomes. We are looking to expand the study with a collaboration with a local cardiology practice to take a more detailed look at clinical outcomes as well as the safe use of anti-hypertensive drugs.
Patient

Andrew (alias used)
Andrew completed an ABPM study through the pharmacy based-service after a recommendation from his primary care physician.
Were you previously diagnosed as hypertensive?
My primary care physician told me that my blood pressure was high, so he put me on a low dose of medication. I was also told I have white coat syndrome and that my blood pressure was very high when I went to the doctor, but my home measurements were normal.
What led to you taking part in the study?
I heard of the service through my wife, who works at a pharmacy and asked my doctor whether I should have an ABPM study done. My doctor recommended that I should go ahead with the 24-hour study.
How was the process of taking part in the study?
I made an appointment and when I arrived, I was fitted with the device and the pharmacist explained the process to me.
How was the experience of wearing the monitor for 24 hours?
It didn’t bother me at all and although I heard it a couple of times during the night, it didn’t keep me up.
How did the results help you?
I talked with the pharmacist after the end of the study about my report. She showed me the blood pressure report and explained that I had some blood pressure spikes during the night. She also sent the report to my primary care physician.
The report was easy to understand. I was surprised that my blood pressure was spiking during a time I would normally consider a calm period overnight and in the morning while my blood pressure during the day was normal.
Would you recommend having an ABPM study done?
Yes, I would because how do you know unless you know? The report told me that my blood pressure was high at certain times of the day and I can be more attentive to that. I was only using my home blood pressure monitor once a day, so I never knew about my pressure changing.
Pharmacist

Mary Curtis, PharmD
Mary coordinated ABPM studies at the Bremo Pharmacy located within Henrico Hospital in and reviewed results with patients.
How did you get involved in the study?
We have worked with Dr. Dixon previously and knew he was looking for local pharmacies to participate in a study. We are an independent pharmacy within the hospital, so we have a good referral system with other departments.
I personally have high blood pressure and a family history of heart failure. It’s always been a personal thing for me to talk with patients about blood pressure before they were discharged and how we can help patients to live their best life.
We often have contact with patients with hypertension and heart disease either at the bedside within the hospital or counseling patients with hypertension and offering guidance on their medication. All pharmacists within our company have clinical backgrounds and we aim to do more with our patients.
A Success Story
A middle-aged male with a history of normal blood pressure had just started running marathons when he began to have elevated readings, escalating to the point where he had an episode that ended up in the ER. Although he was discharged without finding any major issues, he was referred to have an ABPM study done.
When he came back in, we discussed his results, which were extremely high. We discussed his training, what supplements he was using, etc. The sodium content of his refueling product was extremely high. The patient was also increasing his salt intake with restaurant salt packets to help with his recovery after marathons.
I called his doctor and asked for an immediate appointment to tackle these issues with the patient. The patient came back and let me know he had started working with a personal trainer and was back to running with normal blood pressure.
How has using ABPM changed the way you working with patients?
Many patients are unsure or scared about blood pressure because they have conflicting readings, with high readings taken at the doctor’s office but normal readings at home. The monitor has allowed us to have a conversation with the patient starting with what the BP data look. The physicians also love getting the reports. It’s awesome that they have something that shows the full picture. We’ve had sleep studies previously, but this is the first time we’ve had this available for blood pressure.
Although we’ve had home readings previously, there’s a lot of room for error. With the Oscar 2 it's great to be able to see specific periods where blood pressure is high.
How do you communicate with the patient at the end of the study?
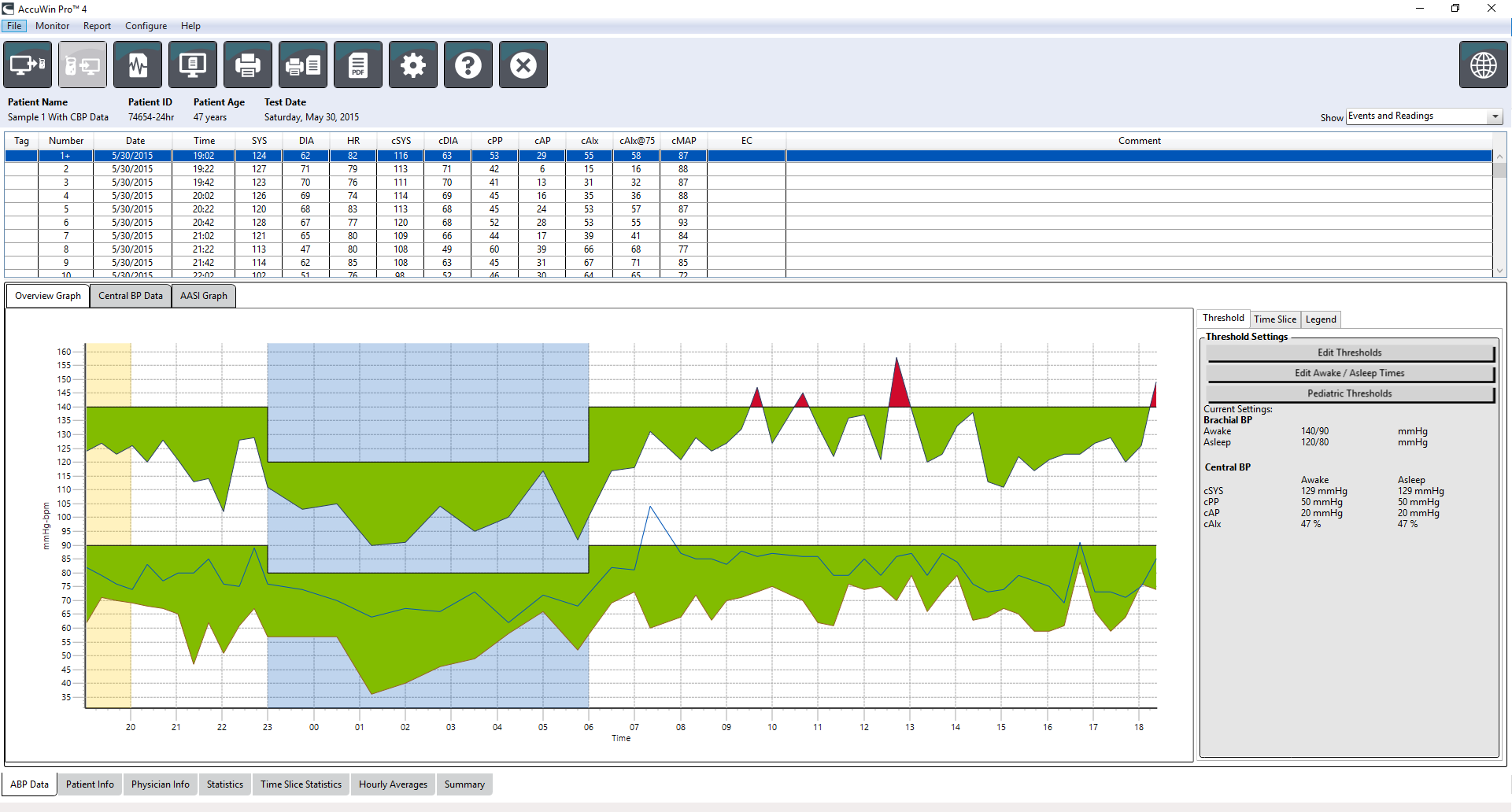
We use the software to pull up the graph and talk about the red and green colored areas. We will reference their physician’s goal for them and show them how they compare. Although it’s not always what the patient wants to hear, especially for patients with high blood pressure, it’s reassuring to have a complete picture that their physician can use to manage their treatment.
“Physicians have loved getting the reports. It’s awesome that they have something that shows the full picture. This is the first time we’ve had this available for blood pressure.”
AccuWin Pro 4 software
[Click to Enlarge]
How has it helped Patients?
We have had multiple patients that were very typical of having White Coat Hypertension. The patients were on medication and came back with readings of low blood pressure. One patient in particular was having dizzy spells on medication and the report came back showing that at certain times the patients were below normal safe limits, which we passed on to the patient’s physician.
How was ABPM tolerated by your patients?
Almost all patients tolerated the experience very well. The occasional patient would report being woken up by readings and a couple of patients discontinued the study. Typically, I was able to coach them using my experience of going through ABPM, I could reassure the patient that it’s only 24 hours and will provide extremely useful data to help manage their blood pressure.
How did you incorporate ABPM into your daily workflow?
It was extremely easy. The physicians would pass on the referral paperwork and we would contact the patients to schedule an ABPM study.
The software was some of the easiest I’ve ever used. We were quickly and easily able to program the monitor and retrieve the data. It was also very easy to bring up the graphs to share with the patients.
Having adequate devices was extremely important for scheduling. There were days we would get 5-6 referrals and having multiple devices available made it much easier to schedule patients at convenient times.
Would you recommend the Oscar 2?
Yes. I wore the monitor myself because I wanted to understand my blood pressure. The device is small, quiet, and easy to wear, and the cuff is comfortable for patients. From the clinical perspective, it has been a great tool to assist with patient care.
